You are about to visit a Philips global content page
Continue
Aug 07, 2021
By the Philips Foundation team

Completing that last mile to connect people living in remote communities with their formal health system is often a challenge in limited-resource settings. Long distances to health facilities, a shortage of professional healthcare workers, and lack of medication or other critical healthcare amenities lead to inadequate community-based care. According to the World Health Organization (WHO), 18 million more health workers are needed to achieve universal healthcare (UHC) in low and lower-middle-income countries. Philips Foundation is exploring ways to empower community health workers with tools, technologies, and skills that enable them to perform more advanced tasks, boost their motivation and increase their capacity to help bridge existing health gaps.
July 2021, we brought together the results and insights from similar projects on how (technological) solutions can enhance the role of community health workers in last-mile healthcare delivery. We discussed them in an informative webinar, recognizing it is essential to collectively explore what works, share lessons and develop effective models that can be scaled to greater impact. Key outtakes and learnings from this dialogue and recommendations to take forward are shared below. For more info on our webinar series, click here.
“Here comes the doctor,” shout a group of children when Abdikadir Dido wipes the dust from his coat and nods goodbye to the motorbike rider who brought him to Golla, a small village near the border of Kenya and Ethiopia. To reach Golla, Dido journeyed 17 km over the red sandy plains of Marsabit. This vast, empty province in northern Kenya is home to sparse settlements and a considerable nomadic community who move along with their cattle, following the seasonal shift of available water and fresh grass. Dido has been a frequent guest of the village for years. As a community health worker, he visits families, educates them about the importance of hygiene and healthy nutrition, checks on childhood diseases, and makes sure children get their vaccines on time. He talks to pregnant women about the importance of going to the nearest primary health facility for regular checks on potential complications. Like many colleague health workers, he is the indispensable provider of basic health services, as well as the entry point into the healthcare system for villagers in remote and underserved areas. However, recently Dido’s status in the Northern tip of Kenya has risen substantially. Since he joined the Save a Mother initiative of Abrassa Mentorship and Empowerment Network (AMEN), led by Marsabit’s First Lady, Rukia Abdulkadir, Dido can do more than promote good health and attend to basic health needs. Today, he comes equipped with a backpack full of diagnostic devices, from a contactless thermometer to a blood pressure monitor and an automated respiratory rate counter. The devices can help him distinguish between malaria and pneumonia, two common childhood illnesses with similar symptoms but different treatment needs. The kit also allows him to investigate suspicions of at-risk pregnancies or early diabetes development by measuring indicative vital signs. Dido is quite pleased with these new tools. “The technology in the backpack allows me to provide my community with healthcare services for which they would previously have to travel for hours,” he says. “It has enriched my job a lot as well.”
The technology in the backpack allows me to provide my community with healthcare services for which they would previously have to travel for hours

It is a scene that Abdulkadir presented during the webinar to illustrate how community health workers can be empowered with the right tools. The outreach kit was part of an integrated community-based health strengthening approach she led in a 2-year project with the Philips Foundation, which focused on enhancing the role of community health workers. In addition to making technology available, health workers were trained and mobilized to collect and use health information data systematically. According to Abdulkadir, the project enabled community health workers to deliver their tasks more effectively. “It enhanced their confidence levels, augmented their earlier education and increased community acceptance. This has led to concrete improvements in outcome in terms of household visits, referrals, demand for services and skilled birth attendance.” Indispensable, yet underutilized Universal healthcare coverage is still a far cry from being realized. With half of the world population still lacking access to essential health services, it is estimated that a total of 18 million health workers will be needed to meet at least that minimum quality of care [1][2]. There is widespread consensus [3] that the highest impact can be reached with community and population-based care, as this can cover the majority of healthcare needs, including prevention, early diagnosis, treatment, rehabilitation, and palliative care. Community health workers play an indispensable role in strengthening community and population-based healthcare throughout the world. People with basic qualifications or limited health backgrounds can be effectively trained and equipped to undertake selected tasks of professional health workers. Working as volunteers in the community, on stipends or with other forms of informal support, community health workers help bring healthcare to communities that otherwise would not receive it, and at the same time, they relieve the burden on overstretched professional health workers. Despite their informal status, community health workers can significantly impact patient health, such as improving outcomes of mother and child care or addressing the increasing burden of non-communicable diseases, such as cancer, diabetes, or heart conditions. Yet despite their recognized significance, the potential of community health workers is underutilized. They are often poorly equipped and lack necessary training and education. In addition, limited payment and career prospects can lead to retention challenges. Can technological solutions help change that? We believe so. It’s all about behavior change In a country-wide campaign of Save the Children in partnership with the national and state governments to fight childhood pneumonia in India, community health workers [4] play a key role in educating rural villages about prevention, as well as recognizing symptoms and seeking care in case of suspicious signs. In a project with Philips Foundation and the Philips India CSR program, Save the Children is now pioneering the use of mobile digital health tools to support community and next-level health workers in these important and educational tasks, as well as with subsequent management of positive cases.
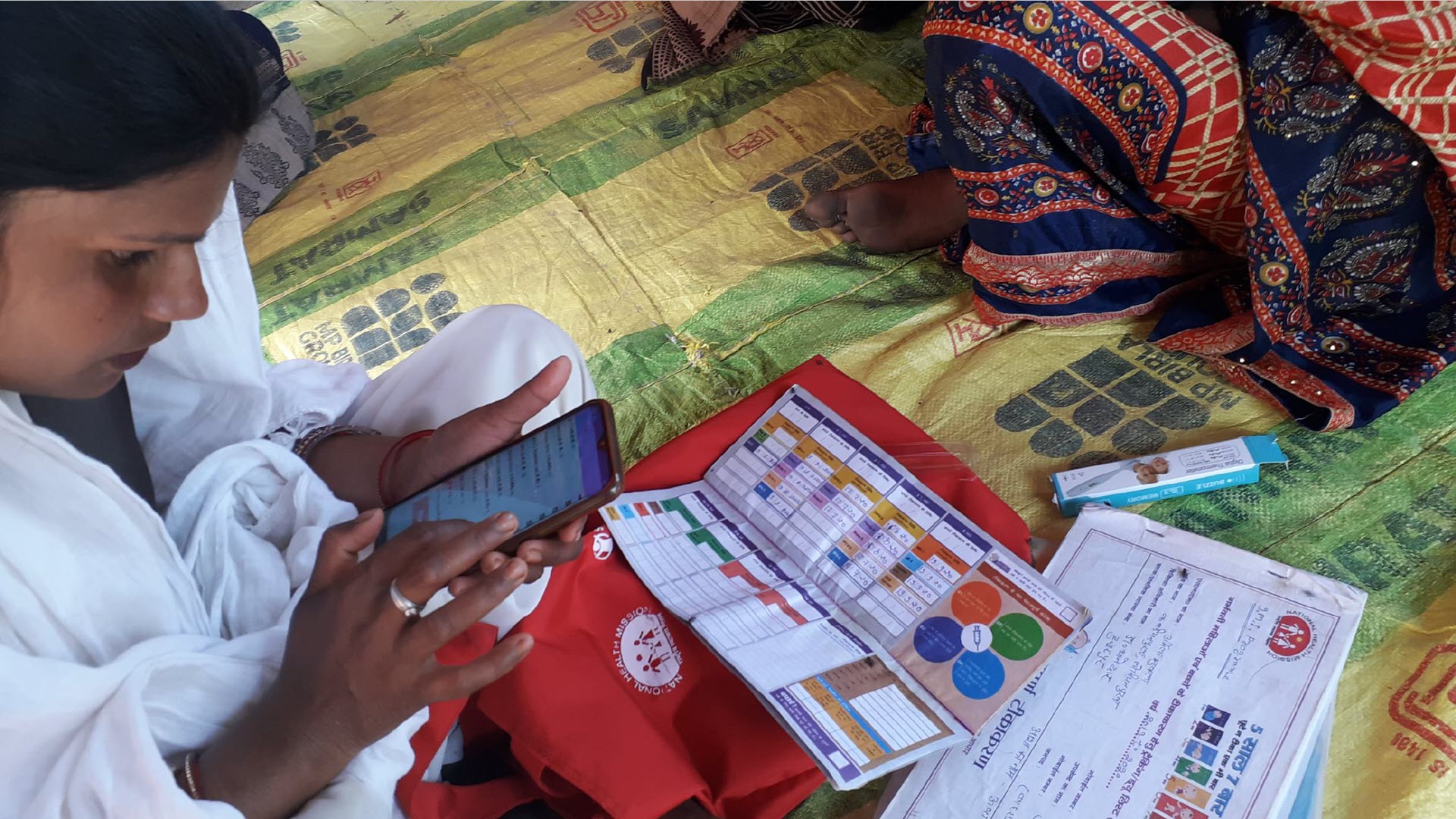
What we see is that through the tools, [health workers] not only get digitally empowered, it also gives them a new face and role in the communities
Dr. OP Singh
Program Management Head Health & Nutrition at Save the Children India
Dr. OP Singh, Program Management Head Health & Nutrition at Save the Children India, oversees the project that has so far involved over 140 [health workers] in rural and urban areas of Rajasthan and Uttar Pradesh, provinces located in northern India. “What we see is that through the tools, [health workers] not only get digitally empowered, it also gives them a new face and role in the communities,” says Singh. “They report that the tools give them more confidence and make them more trusted in counseling, both towards families and community groups. The standard protocols provided make it easier for them to register, classify, assess and refer cases consistently. We do already see that the perceived improvement in quality-of-care results in an increasing demand for their services.” According to Singh, “The aim was to achieve behavior change of people towards better prevention, recognition and case management. I am pleased to see that [health workers] are able to use the tools to influence decision making at the household and caregiver level in their communities. It clearly improves their role in the system of pneumonia management. And the adoption spreads by word of mouth. More and more [health workers] who have not used digital tools before are motivated by seeing how it works with their peers, and they seek help to get up to speed.” Similar experiences were observed in a project with Kenya Red Cross. The project aimed to validate a high-risk pregnancy awareness tool previously co-developed by Philips Foundation and the International Committee of the Red Cross (ICRC). Initially designed as paper-based booklet to serve in fragile environments with poor (digital) infrastructure, the tool also proved valuable in more stable and varied settings such as rural Kenya, stimulating conversations between community health workers and pregnant women about risk factors and healthy habits around pregnancy.
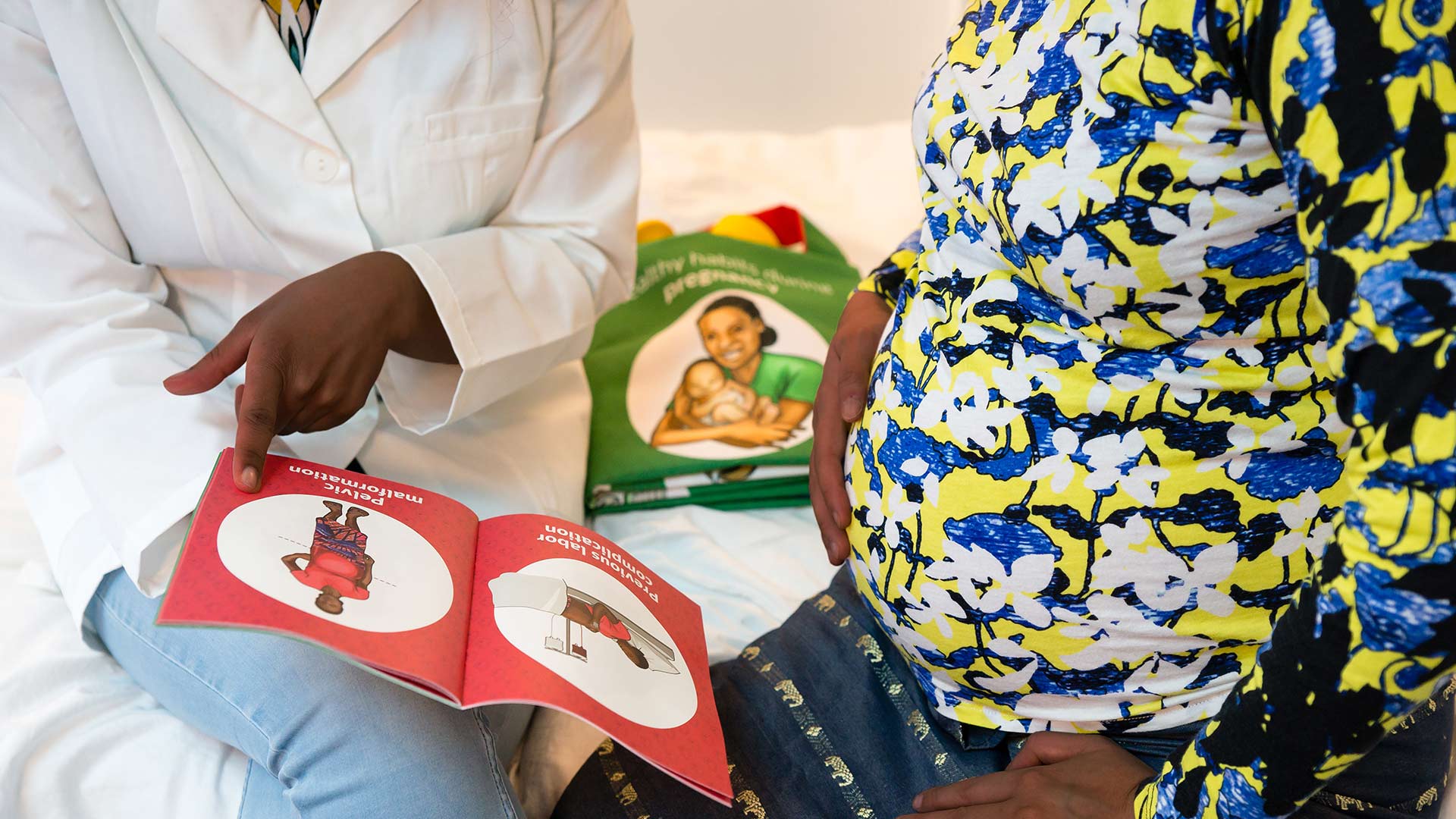
In a scientifically designed research project reaching over 250,000 people, the high-risk pregnancy awareness tool was shown to be effective in increasing the general level of knowledge – from health workers to pregnant women, as well as traditional attendants, such as husbands, partners, and mothers (in law), who were often directly involved in pregnancy guidance and decision making. As a result, the project increased identification of at-risk pregnancies, utilization of antenatal care services offered by health facilities, skilled deliveries, and referrals from the community to primary or higher levels of care. Sarah Kedenge, a scientist at Philips Research in Nairobi who conducted large parts of the scientific study, adds: “What was interesting was that the tool was embedded into and was seen to add value to the existing structure and routine activities around pregnancy care. This enriched the role of community health workers and strengthened their position in the end-to-end health referral system. I also see this as the way to scale up. It’s not a stand-alone intervention that needs heavy resources to be implemented; it can actually add value to the systems already in place.” One of the pointers of the project was the potential use of digital tools in addition to paper-based ones, but is there a preference and why? Design for inclusion The key question is how design can play a role in developing healthcare solutions in resource-limited settings. Paper or digital, Dr. Simona Rocchi, Senior Director at Philips Experience Design, sees the value in both. “It really depends on the setting,” she says. “Design for inclusion in access to healthcare means shaping people-centric tools that can empower community health workers in their social fabric to perform their tasks and use their presence more effectively. But they are often under-equipped and little trained. Paper tools can be the best choice to let them perform best in settings with no or very limited availability of electricity and connectivity.” According to Rocchi: "In designing the best tools, you need also to understand the health workers’ requirements, their target group, level of education and knowledge in relation to technology. The infrastructural and cultural reality on the ground matters just as much. When we developed the high-risk pregnancy cards, the International Committee of the Red Cross (ICRC) made it clear to us that in visualizing the pathological aspects of pregnancy complications, in some cultures, it would hamper uptake if uncovered parts of the body would be shown in the images.”
Design for inclusion in access to healthcare means shaping people-centric tools that can empower community health workers in their social fabric to perform their tasks and use their presence more effectively
Dr. Simona Rocchi
Senior Director at Philips Experience Design
Participants in the webinar stress the importance of understanding the local context. This means considering in the design any language, technology, or digital and health literacy barriers of healthcare workers and the communities they serve. These factors can affect the implementation or effectiveness of the tools. The Netherlands Red Cross’ global 510 Initiative, for example, is leading an ambitious program of digital and data-driven innovation of humanitarian aid. One of its elements is a safe, fast, and fair cash-based aid program to help people affected by disaster meet their most urgent needs. Nowhere is the need for equitable access and the risks of technical errors greater than in programs aimed at providing cash to people in disaster-stricken areas. Despite the challenges, Orla Canavan, strategic product design lead for the 510 Initiative, doesn’t shy away from digital tools. “It could have been a consideration to use paper from the point of view of the people applying for aid. However, from the perspective of the aid workers and the Red Cross organization, it was clear from the start that only a digital system could bring us the step forward we wanted to make, by giving us the ability to register people safely, equitably and with dignity and allowing us to distribute cash in a safe manner.” Therefore, the 510 Initiative has listened extensively to and tested with target users to develop user-friendly digital interaction methods. In Kenya, for example, the team decided to use voice-activated menus in the local language, asking one question at a time and providing the option for answers to be read aloud. People could then select from the menu with a simple touch of a button. Users received a brief training and could get assistance from community volunteers in using the system – a combination that worked well. But inclusive design does not stop at the user interface. “Deployment strategies need to be an integral part of it,” stated Ayushi Singh. She is a program manager at ZMQ, an India-based social enterprise that is fully dedicated to creating digital solutions for behavior change communication and connecting communities to health services in the last mile.

“We always start solution design through participatory interaction on the ground. We use methods like story labs, stage plays and group sessions to try out prototypes to deeply understand the needs, social-cultural background, and the use and acceptance of technology. Only then do we put the final digitization in place and use techniques to enhance engagement, such as storytelling and gamification.” ZMQ is an advocate for the use of technological or digital solutions to facilitate the work of community health workers and improve access to quality care. Their approach and the successful implementation of their mobile health solutions have been deployed in geographies as diverse as India, Afghanistan and Uganda. What underlies this approach? Technology for retention The widespread deployment of community health workers can be both a blessing and a vulnerability when it comes to making primary healthcare systems more resilient and sustainable. On the one hand, community health workers help address the shortage of human resources for health in limited-resource settings and bridge the last-mile healthcare gap. On the other hand, the volunteer status or low-pay nature of the role leads to high attrition rates and continuous recruitment, education, and retention challenges to ensure the sustainability of services. Therefore, insight into motivation drivers and solutions that can boost retention is of great interest to organizations that aim to strengthen community-based care. This prompted the International Federation of Red Cross and Red Crescent Societies (IFRC), the Finnish and Kenya Red Cross Societies, and Philips Foundation to explore how performance-enhancing and technical solutions could motivate community health workers to remain active in the system. In the study, a group of community health workers received the same outreach kit used by Dido in Marsabit county. The effect on motivation in this group was similar to other workers who receive incentives unrelated to their role in the health system, such as skills to establish a stable livelihood. “The study proved that technology provision was indeed a motivator,” said Irene Adema, a scientist from Philips Research Kenya, who led the research.
Community health workers are very much intrinsically motivated, driven by the ability to deliver quality health services to their community. It’s encouraging to see that technologic solutions can be an enabler for that
Irene Adema
Scientist from Philips Research Kenya
“We saw that the outreach kit ranked highest among other incentives, even above stipends, for the intervention group. It also had a ripple effect on other factors known to motivate healthcare workers, such as training and skills development, recognition, community trust, and linkage to the health facility. To me, it shows that community health workers are very much intrinsically motivated, driven by the ability to deliver quality health services to their community. It’s encouraging to see that technologic solutions can be an enabler for that.” Philips Foundation also saw this reflected in the work of social enterprise Healthy Entrepreneurs. When, many years back, Joost van Engen traveled through Africa selling canned meat, it struck him that global supply chains were able to deliver commodities to the most remote outposts in the continent, but healthcare failed to do so. That inspired him to establish Healthy Entrepreneurs, a social business working from Uganda that enables community health workers to become small business owners, sell essential medicines and health products, and disseminate information.

“By optimizing and scaling supply chains, we enable these community health workers to do what they are supposed to do, but in a financially sustainable way. We make them ‘community health entrepreneurs,’” Joost explained. With 6,000 franchise holders already in Uganda, the model is growing fast and expanding to other countries. His standard model is supply chain based: buying and selling commodities in bulk. Together with Philips Foundation, Healthy Entrepreneurs explored a model to expand their services to include diagnostic tools, more complex consults and follow ups. Done through a “doctor at a distance” telehealth model, 50 community health workers were empowered by receiving support from a doctor in the office via an app-based collaboration and data-sharing platform. The model has proven to work well in increasing disease awareness, expanding access to healthcare services, lowering patients’ healthcare costs and increasing revenues for the participating community health workers. For some the extra income allowed them to quit side jobs or to pay for the school fee of their children, so really a significant difference. Where next? 2021 has been designated by WHO as the International Year of Health Workers as a token of appreciation and gratitude for their relentless efforts in the fight against the COVID-19 pandemic. It just goes to show how fundamental this work can be, and thus we cannot ignore the indispensable role of community health workers in last-mile delivery and building resilient healthcare systems. The results discussed in this article show that it is possible to strengthen their role, impact, motivation and income by providing them with the smartly chosen tools and technology. But how do we deploy these results from pilot projects and longitudinal studies on a larger scale so that a mass impact can be generated without the need for unsustainable funding? Webinar participants agreed that if tools that enhance outcomes can be embedded into existing systems, everyone benefits without adding costs. A mix of top-down and bottom-up engagement practices is needed to secure both compatibility and coordination from a health systems governance point of view and making sure the solution is accepted and appreciated by the individual people who seek better access to healthcare. Similarly, scaling comes with the need to develop standardized approaches that allow for robust replication, while also requiring that solutions are sufficiently customized to meet individual needs.

Philips Foundation continues to explore what is needed to achieve greater scalable impact and remains committed to strengthening community health, which provides the foundation for universal access to quality healthcare for all. That's why in our next webinar of a series, we'll take a deeper look at the scalability of healthcare models, and how digitization and social entrepreneurship can be the driving forces.
By optimizing and scaling supply chains, we enable these community health workers to do what they are supposed to do, but in a financially sustainable way. We make them 'community health entrepreneurs'
Joost van Engen
Founder of Healthy Entrepreneurs
[1] 18 million more health workers are needed to achieve universal healthcare (UHC) in low and lower-middle-income countries (who.int) [2] World will lack 18 million health workers by 2030 without adequate investment, warns UN (who.int) [PDF] [3] Strengthening primary health care through community healthworkers: Investment case and financing recommendations (who.int) [PDF] [4] In India, community health workers are referred to ASHAs, acronym for Accredited Social Health Activists. In this paper, we chose to stick to ‘community health workers’ to avoid any confusion.
June 16, 2026
April 24, 2026
March 10, 2026
January 28, 2026
December 11, 2025







